 In the cervical, thoracic, and lumbar spine, all vertebrae are essentially similar. Each
In the cervical, thoracic, and lumbar spine, all vertebrae are essentially similar. Each 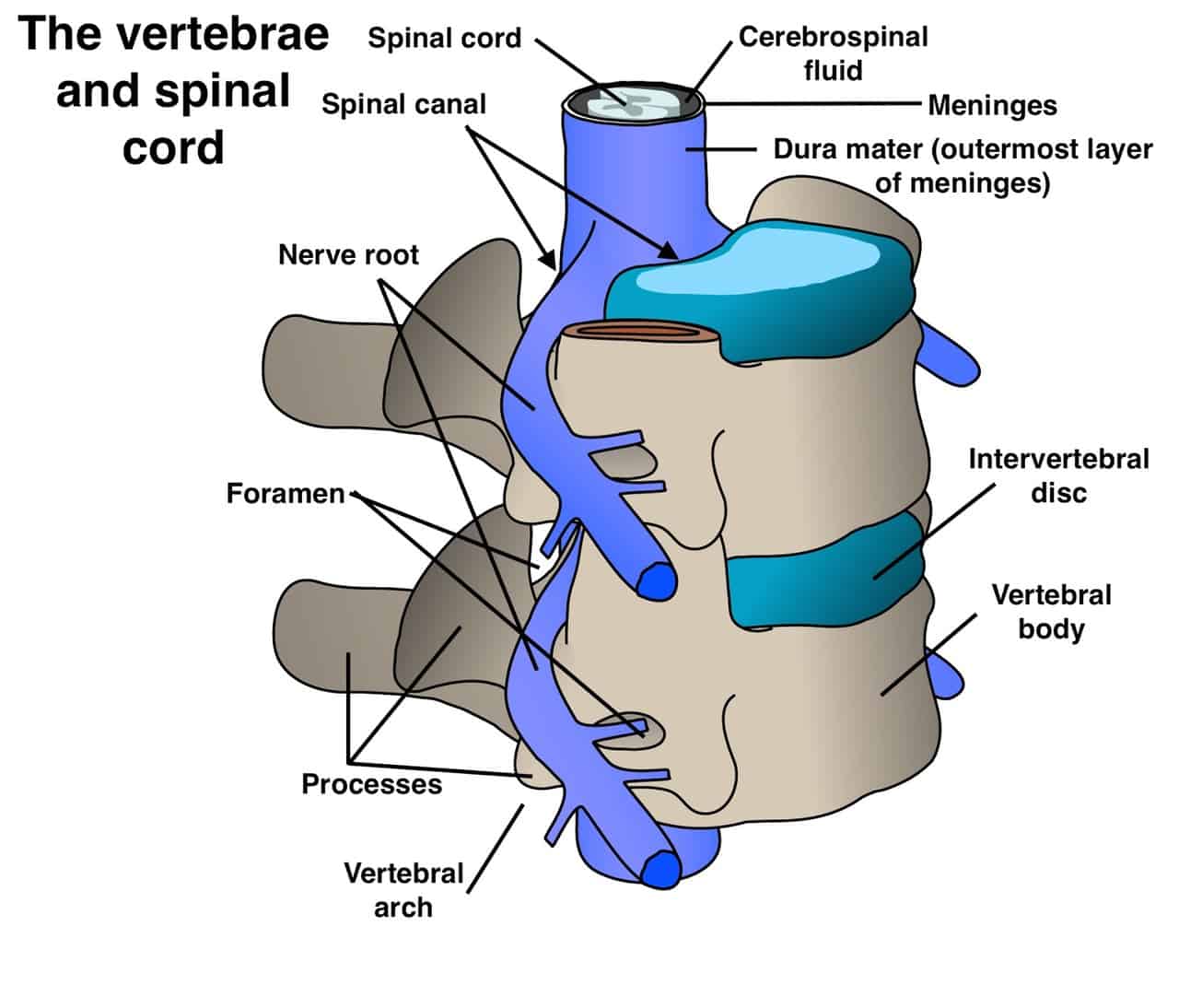
Dr. McCormick named as one of Castle Connolly’s Top United States and New York Doctors/Neurosurgery for 25 consecutive years.
| Header | Text |
| Treatment Options | Many spinal conditions respond well to surgical treatment. In properly selected patients, surgery provides relief of symptoms, returns function, halts neurological damage, and achieves or restores spinal stability for most patients. At the Spine Hospital at the Neurological Institute of New York, we pride ourselves on providing our patients with clear explanations and the best possible surgical outcomes. The highly trained neurosurgeons in our practice continue a long tradition of expertise, skill, and care, which consistently places them among the top neurosurgeons in the country. However, surgery is not the treatment of choice for every patient with every condition. The experienced neurosurgeons at The Spine Hospital at the Neurological Institute evaluate each case individually and will tailor a nonsurgical or surgical treatment plan to each patient. To read more about a particular condition and its general treatment options, have a look at our conditions pages. |
| Spinal Anatomy | To understand how problems of the spine are treated surgically, it helps to understand the structure of the normal spine.
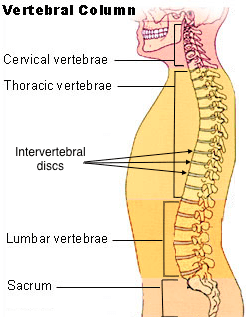
The spine is composed of many vertebrae, or individual bones of the spine, stacked one on top of another. Together, this stack forms the vertebral column. The topmost section of the vertebral column, the section in the neck, is called the cervical spine. The next section, located in the upper and mid-back, is called the thoracic spine. Below the thoracic spine is the lumbar spine, in the lower back. Finally, the sacral spine (or sacrum) is located below the small of the back, between the hips. Sturdy intervertebral discs connect the vertebrae. The intervertebral discs act as cushions and shock absorbers between the vertebrae. Each disc is composed of a jelly-like core surrounded by a fibrous outer ring.
|
| Glossary | Names of surgical procedures often include terms related to anatomy (body structure) or surgery. Understanding those terms can help patients make sense of the name of a surgical procedure. ANATOMICAL:
SURGICAL:
|
| Preparing for Your Appointment | At The Spine Hospital at The Neurological Institute of New York, our neurosurgeons want you to feel as prepared as possible for your surgery. We want to make sure you understand the goals of your procedure, as well as what you can expect following the surgery. The information on this site can help you understand your condition, its general surgical treatment, and how to prepare for surgery in general. For example: make a list of your medications and allergies for your doctor; do not wear nail polish or makeup on the day of surgery. But your neurosurgeon is the very best resource for helping you understand the ins and outs of your individual case, so use your time with him or her at your appointment to ask questions. Some patients find it helpful to write down questions as they think of them, and bring those lists of questions to their appointments. The world-class neurosurgeons at The Spine Hospital at The Neurological Institute of New York continue a long tradition of skill, care, and expertise that result in the best possible surgical outcomes for our patients. Drs. Paul C. McCormick, Michael G. Kaiser, Peter D. Angevine, Alfred T. Ogden, Christopher E. Mandigo, Patrick C. Reid and Richard C.E. Anderson (Pediatric) are experts in surgical spine treatments.
|
Helpful Surgery Overviews
Dr. McCormick will choose the treatment method specific to each patient and situation. Some of the condition’s treatment options may be listed below.
Recent News
Dr. McCormick named as one of Castle Connolly’s Top United States and New York Doctors/Neurosurgery for 25 consecutive years.

Dr. McCormick participated as both a member of the expert panel as well as a co-author of recently published randomized study on the treatment of grade 1 degenerative spondylolisthesis. This condition commonly occurs in adult patients and is subject to numerous types...

Dr. McCormick was invited to present his experience on the evaluation and microsurgical management of intramedullary spinal cord tumors. Dr. McCormick described his techniques and illustrated on video the safe and complete microsurgical resection of both an...