Dr. McCormick named as one of Castle Connolly’s Top United States and New York Doctors/Neurosurgery for 25 consecutive years.
| Header | Text |
| What is a Cervical Laminectomy? | Cervical = having to do with the spine in the neck 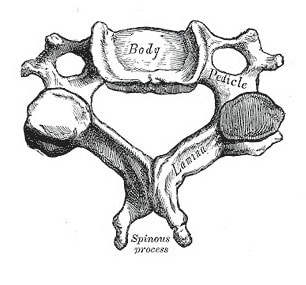 A cervical vertebra. Note the lamina, the flat section of bone near the spinous process. Image Credit: Henry Gray, Anatomy of the Human Body, Public Domain.
|
| When is this Procedure Performed? | A cervical laminectomy is performed for certain patients with cervical spinal stenosis, which is a narrowing of the spinal canal. Stenosis may be caused by a number of degenerative spine conditions, including wear and tear on the bones, discs, and ligaments. A narrow spinal canal can compress (pinch) the spinal cord and surrounding nerves. Compression may irritate a spinal nerve or nerves, causing radiculopathy (pain, weakness, numbness or tingling in one limb). Compression of the spinal cord itself can damage its delicate tissues and cause myelopathy (pain, weakness, numbness or tingling in both arms or legs, difficulty walking, and/or loss of bowel or bladder control). A laminectomy decompresses (removes the pressure from) the spinal cord and spinal nerves. It is generally effective when performed in patients who have an identifiable compression resulting in radiculopathy or myelopathy. Before surgery is considered, nonoperative measures like physical therapy and pain medications may be tried. These measures provide effective relief in many cases. But when other treatment plans do not provide relief, and a problem exists that can be surgically corrected, surgery is often the treatment of choice. Surgery is also typically required for cases in which the spinal cord is compressed. Like any other surgical procedure, a cervical laminectomy entails a certain amount of risk. However, the procedure is generally safe, and the risks are usually small. Patients typically derive great benefit from the procedure. |
| How is this Procedure Performed? | A cervical laminectomy is performed under general anesthesia. An incision is made down the middle of the back of the neck to allow the surgeon to access the back of the cervical spine. The surgeon then removes the lamina. Removing the lamina relieves the pressure on the spinal cord. The “roof” of the spinal canal is left open; the lamina does not need to be replaced by a plate or bone graft. If necessary, pressure on the spinal nerves can be relieved with a procedure called a foraminotomy. In this procedure, the surgeon removes some bone from the joint (called a facet joint) that compresses the nerve. A foraminotomy is often performed at the same time as a laminectomy. After a laminectomy, the surgeon may perform a spinal fusion to ensure the spinal column is stable. During a spinal fusion, the surgeon inserts a bone graft to join two or more of the affected vertebrae together into a single unit. In some cases, the surgeon may use instruments such as a metal plate and screws to hold the bones in place until they heal. Finally, working layer by layer, the surgeon will close the incision using absorbable sutures (sutures that can be dissolved by the body and do not need to be physically removed). |
| How Should I Prepare for this Procedure? | Make sure to tell your doctor about any medications that you’re taking, including over the counter medication and supplements, especially medications that can thin your blood such as aspirin. Your doctor may recommend you stop taking these medications before your procedure. To make it easier, write all of your medications down before the day of surgery. Be sure to tell your doctor if you have an allergy to any medications, food, or latex (some surgical gloves are made of latex). On the day of surgery, remove any nail polish or acrylic nails, do not wear makeup and remove all jewelry.wigs/hairpiece. Also, you will need to remove contact lenses, eyeglasses, and dentures. If staying overnight, bring items that may be needed, such as a toothbrush, toothpaste, and dentures. |
| What Should I Expect After the Procedure? | Post-surgical pain is usually controlled with intravenous pain medication for the first day, followed by oral pain medication. On average, patients are discharged from the hospital two to three days following surgery. Most patients are encouraged to walk as soon as possible, often on the day of surgery. At home, patients are usually encouraged to increase their activities as they are able to tolerate. A soft collar may be prescribed for comfort in patients in whom a fusion has not been performed. In patients with fusion, however, a firm cervical collar may be prescribed for up to 6 weeks following the surgery. The surgeon will schedule a follow up visit, typically 4-6 weeks after surgery. Physical therapy that focuses on the neck will often be started at the time of the follow up visit. Physical therapy initially involves stretching and range of motion exercises, and then endurance and strength training. Physical therapy may be delayed for an additional 4-6 weeks for patients who have had a spinal fusion. |
| Preparing for Your Appointment | Drs. Paul C. McCormick, Michael G. Kaiser, Peter D. Angevine, Alfred T. Ogden, Christopher E. Mandigo, Patrick C. Reid and Richard C.E. Anderson (Pediatric) are experts in cervical laminectomy.
|
Helpful Surgery Overviews
Dr. McCormick will choose the treatment method specific to each patient and situation. Some of the condition’s treatment options may be listed below.
Recent News
Dr. McCormick named as one of Castle Connolly’s Top United States and New York Doctors/Neurosurgery for 25 consecutive years.

Dr. McCormick participated as both a member of the expert panel as well as a co-author of recently published randomized study on the treatment of grade 1 degenerative spondylolisthesis. This condition commonly occurs in adult patients and is subject to numerous types...

Dr. McCormick was invited to present his experience on the evaluation and microsurgical management of intramedullary spinal cord tumors. Dr. McCormick described his techniques and illustrated on video the safe and complete microsurgical resection of both an...