Dr. McCormick named as one of Castle Connolly’s Top United States and New York Doctors/Neurosurgery for 25 consecutive years.
| Header | Text |
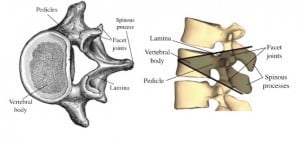
| What is a Pedicle Subtraction Osteotomy (PSO)? | Pedicle = a section of bone that connects the front and back of a vertebra |
| When is this Procedure Performed? | When viewed from the side, a typical spine has a few gentle curves that balance each other out, aligning the body’s center of gravity over the pelvis. This alignment is called sagittal balance. Conditions like hyperkyphosis, ankylosing spondylitis, and flatback syndrome can put the body’s center of gravity too far ahead of the pelvis, resulting in sagittal imbalance. Pedicle subtraction osteotomy is one surgical option for treating sagittal imbalance. Image credit: |
| How is this Procedure Performed? | A pedicle subtraction osteotomy is performed under general anesthesia, which means the patient is unconscious. Spinal cord monitoring techniques like SSEP (somato-sensory evoked potentials) and MEP (motor-evoked potentials) measure electrical activity in nerves and help ensure the safety of the spinal cord throughout the operation. Once the patient is unconscious, he or she is carefully placed face-down on a special hinged operating table. The table is set up something like an upside-down flattened letter “V”, where the tip of the V points up towards the ceiling. (The table is much flatter than an actual upside-down letter “V”.) An incision is made in the center of the back and the bones of the spinal column are exposed. Then the surgeon places screws in the vertebrae above and below the targeted area. These screws are called pedicle screws because they are inserted into the pedicles–the thick, sturdy columns of bone that connect the back of the vertebra with the front. Later in the surgery, the pedicle screws above and below the target vertebra will provide attachment points for the rods that will hold the spine in position while it heals. Next the surgeon removes the projections, called processes, from the back of the target vertebra. The surgeon hollows out a space under the pedicles of the target vertebra, removing the pedicles. Then the surgeon enlarges the space, creating a wedge-shaped hollow space in the vertebra. Once the wedge-shaped hollow is complete, its upper and lower portion can be brought together. This closes the wedge and provides about 30 degrees of correction to the deformity. The surgeon gradually widens the special surgical table from its reverse “V” into a flatter position, until the bone surfaces lie against each other and the wedge is closed. Finally, rods are placed in the pedicle screws to help hold the spine in position while it heals. As the bone surfaces of the upper and lower wedge grow together, permanently fusing into one solid bone, they will provide lasting strength and stability to the vertebra. |
| How Should I Prepare for this Procedure? | Before any deformity correction surgery, it is important to stop using tobacco products. Nicotine has a very detrimental effect on bone fusion and surgery outcomes. If you currently smoke or use tobacco, speak to your neurosurgeon about quitting. Be sure you understand the goals of your or your child’s surgery, the risks, and what can be expected from the recovery period. If you have any questions at all about the procedure or the recovery, speak with your or your child’s neurosurgeon. To make it easier, write down your or your child’s questions as they arise, and bring the list to your appointments. Make sure to tell your doctor about any medications or supplements that you or the patient are taking, especially medications that can thin your blood such as aspirin. Your doctor may recommend you or the patient stop taking these medications before your procedure. To make it easier, write all medications down before the day of surgery. Be sure to tell your doctor if you or the patient have an allergy to any medications, food, or latex (some surgical gloves are made of latex). On the day of surgery, remove any nail polish or acrylic nails, do not wear makeup and remove all jewelry. If staying overnight, bring items that may be needed, such as a toothbrush, toothpaste, and dentures. You will be given an ID bracelet. It will include your name, birthdate, and surgeon’s name. |
| What Should I Expect After the Procedure? | How long will I stay in the hospital? Will I need to take any special medications? Will I need to wear a brace or collar? When can I resume exercise? Will I need rehabilitation or physical therapy? Will I have any long-term limitations due to a pedicle subtraction osteotomy? |
| Preparing for Your Appointment | At The Spine Hospital at the Neurological Institute of New York, Drs. Paul C. McCormick, Michael G. Kaiser, Peter D. Angevine, Christopher E. Mandigo and Patrick C. Reid are experts in pedicle subtraction osteotomy. Dr. Richard C. E. Anderson is an expert in pedicle subtraction osteotomy for pediatric patients. |
Helpful Surgery Overviews
Dr. McCormick will choose the treatment method specific to each patient and situation. Some of the condition’s treatment options may be listed below.
Recent News
Dr. McCormick named as one of Castle Connolly’s Top United States and New York Doctors/Neurosurgery for 25 consecutive years.

Dr. McCormick participated as both a member of the expert panel as well as a co-author of recently published randomized study on the treatment of grade 1 degenerative spondylolisthesis. This condition commonly occurs in adult patients and is subject to numerous types...

Dr. McCormick was invited to present his experience on the evaluation and microsurgical management of intramedullary spinal cord tumors. Dr. McCormick described his techniques and illustrated on video the safe and complete microsurgical resection of both an...